The Help Phase
The Help Phase:
Intervention
INTRODUCTION
Once the factors causing the outcome variable
have been identified and mapped in the process model, the intervention can be
developed. An intervention is a means to change the causal factors and thus the outcome variables in the desired
direction. An adequate intervention targets
one or more causal factors in the process model. Yet often it is not feasible or even necessary to target all variables
in this model. Therefore, the first step in the Help stage of the PATH model is to determine which causal factors
will be targeted in the intervention.
The modifiability of the factors and the expected effect sizes of interventions will direct this choice. Once
these factors have been identified, an intervention
that targets these factors can be developed. Decisions must be made about how the target group will be reached and what the
content of the intervention will be. The
content depends largely on empirical evidence. The last step in the Help phase
concerns the implementation process.
Here care is taken that the intervention is used as intended. We want to emphasize that the present
chapter only gives an introduction into the art of intervention development,
and that more detailed approaches are available elsewhere, for instance, in the context of health education (see for
example, Bartholomew, Parcel, Kok
& Gottlieb, 2006).
It is
known that racial discrimination may have severe psychological consequences for people who are discriminated against: they
may feel unfairly treated, depressed, angry and/or sad. But can racial
discrimination also harm physical health?
In general Black US citizens suffer from higher blood pressure than White US
citizens. Is it possible that this has something to do with racial
discrimination? To answer this
question, researchers Nancy Krieger and Stephen Sidney conducted a study*
among more than 4000 Black and White adults. Participants' blood pressure was assessed, and they were asked
about their experiences with racial
discrimination and their ways of coping with it. They were asked, for
Box 5.1 Case Study: Racial Discrimination
and Blood Pressure
and Blood Pressure
The
Help Phase 107
example,
'Do you accept racial discrimination as a fact of life or do you try to do something about it?', and 'Do you talk to other people
about being discriminated against or do you keep it
to yourself?'.
The
researchers discovered that, surprisingly, among working-class Black men and women, blood pressure was elevated among those who
reported either a great deal of racial
discrimination or no discrimination at all.
According to the researchers this does not mean that
(intermediate) levels of racial discrimination are healthy.lt is, for instance, possible that people who experience discrimination
find it too painful to admit to and, consequently, do not report it as such. It
is also possible that discriminated individuals suffer
from so-called 'internalized oppression', that is, they perceive unfair
treatment as 'deserved' and non-discriminatory.
Furthermore,
the researchers found that the way Black individuals cope with racial discrimination is at least as important as racial
discrimination itself. Among working-class Black men
and women blood pressure was highest among those who responded
to unfair treatment by accepting it as a fact of life, and did nothing about
it.
Krieger
and Sidney's (1996) study underlines that racial discrimination is not just a problem for those who are discriminated against, but
for society as a whole. Having high blood pressure
and falling ill as a consequence of feeling discriminated against may lead to job absenteeism, a loss of
productivity and a rise in healthcare
costs. Moreover, the study suggests that, in addition to anti-discrimination policies aiming to prevent discrimination, the government
might also develop a campaign to encourage
Blacks not to accept discrimination as a fact of life but to become assertive and to claim their right to fair
treatment
*
Krieger, N. & Sidney, S. (1996). Racial discrimination and blood pressure:
the CARDIA study of young black and white
adults. American
Journal of Public Health, 86, 1370-1378.
PREPARING INTERVENTION
DEVELOPMENT
The essence of the final Help phase is that
interventions must focus on changing factors
in the explanatory model. It is not always necessary, appropriate, or possible
to target all the factors in the
explanatory model. Therefore, the applied social psychologist chooses the factors that are modifiable and that have the greatest effect on the outcome variable. To do so, it is convenient to put
all the factors from the process model into a balance table (see Table 5.1).
Modifiability
Although presumably many
variables in the selected process model can be influenced, there may be considerable
differences in the degree to which this is possible. Three questions can help to exclude factors that are
difficult to change:
108 Applying Social Psychology
1.
Does the factor concern a
stable personality
trait? For example, when a psychologist wants to
develop an intervention to tackle shyness, one may include introversion as a
personality variable with a high degree of
explanatory power in the model, but this variable has little potential for change outside intensive
psychotherapy. Or when one includes neuroticism as a variable in a model predicting burnout, one needs
to realize that this is a stable personality trait that will be difficult to
change.
2.
Is the factor related to
deeply held political or religious values? For example, it will be virtually impossible to attract attention for a programme on
condom use from people who, based on
their religious convictions, are strongly against premarital sex. Or it may be
difficult to convince selection officers with very negative
attitudes towards immigrants to endorse a policy to employ people from
minority groups.
3.
Is the factor related to stable environmental
conditions? For example, a problem might be that students
do not park their bikes in the appropriate parking spaces at university.
Perhaps they see many other bikes parked in
inappropriate spaces and follow that example. However, this might be due to insufficient bike storage
facilities on campus, which is a stable environmental condition.
Effect
Size
Not all factors in the process model have an
equally strong impact on the outcome variable, and applied psychologists should focus
on the ones that have the strongest effect. This selection is facilitated
if there is empirical evidence for the strength of the causal relationships
in the model. Often, however, this is not available and psychologists
'guestimate' the effect sizes. Various sources of information can be
helpful to estimate the effects.
Past
Experience with Similar Situations
Suppose
a school aims to tackle cultural segregation among their students.
In the
process
model, the recruited psychologist identifies 'knowledge about people from other
cultures' and 'personal contact with people from other cultures' as factors
predicting segregation. Yet last year the school board decided
to provide youngsters with positive knowledge on other cultures, and,
although students were more positive, this seemed to have no effect
on social interactions in the school. Armed with this knowledge,
it does not seem very sensible to try this strategy again.
Empirical
Evidence
For a number of factors in the model, there
may be empirical evidence that they are resilient to change. For example, the
literature shows that most people are unrealistically optimistic about their
lives (Weinstein & Klein, 1996). Most children, for example,
believe they have less risk than the average child of becoming overweight and
developing health problems as a result of being overweight. As this optimism is
a statistical impossibility — it simply cannot be that most
people are better off than the average person — a psychologist may believe it
could help to educate people about this illusion. However, research suggests that
such biased perceptions are hard to correct and that their influence
on behaviour is limited (Weinstein, 2003). Thus, one would not select
this factor to be targeted in an intervention. In general, it makes sense to
look for evidence showing the degree to which the model variables
are changeable.
The
Help Phase 109

Figure 5.1 Process model: What factors influence weight regulating parental behaviours?
The
Balance Table
A
balance table helps in making the decision on which factors will be targeted in
the intervention. We illustrate the balance table through the
problem of obesity among children in the UK. Britain is one of the 'fattest'
nations in Europe. In 2000, 27 per cent of girls and 20 per
cent of boys aged 2 to 19 years were overweight (see the websites on NationalStatistics,
www.statistics.gov.uk).
Obesity amongst children is a problem of great concern: such children
have a high risk of developing long-term chronic conditions, including
adult-onset diabetes, coronary heart disease, orthopaedic disorders, and
respiratory disease. A social psychologist is asked to develop an intervention
to help tackle this problem. In studying the literature she
discovers that one of the major causes of obesity is the
influence of parents on the weight of their children (Jackson, Mannix &
Faga, 2005), namely, that parents may not do enough to stop weight
gain in their children. Such behaviours are referred to as weight regulating parental behaviours. A
psychologist will develop a process model in which these behaviours
are the outcome variable (see Figure 5.1).
Next, a psychologist will evaluate all the
variables from the process model with regard to their modifiability and their
effect size, that is the magnitude of the impact of the change on the outcome
variable.
110 Applying Social Psychology
Table 5.1 Balance table
Variables from the process model
|
Modifiability
|
Effect
size
|
1.
Perceived negative outcomes of child being
overweight
|
++
|
|
2.
Perceived positive outcomes of weight
reducing parental behaviours
|
++
|
|
3.
Perceived
response-efficacy of child's behaviour to lose
weight (does a change in the child's behaviour lead to
losing weight?)
|
++
|
|
4.
Perceived control over weight reducing
parental behaviours
|
||
5.
Knowledge on weight reducing parental
behaviours
|
++
|
++
|
6.
Perceived control over child's behaviour
|
++
|
|
7.
Experience with structured parenting
|
0
|
|
8.
Positive attitude with regard to democratic
parental style
|
0
|
0
or +
|
Note With regard to modifiability: ++ = high modifiable; + =
medium modifiable; 0 = low modifiable, — = not
modifiable, +/0 = depends on another variable.
With regard to the effect size: ++ = large effect; + =
moderate effect; 0 = small effect; — = no effect +10 = depends on
another variable.
First, she evaluates the modifiability of the
eight causal factors in the process model. The
first three factors — the perceived negative outcomes of a child being
overweight, the perceived positive outcomes of regulating one's
child's weight, the perceived response-efficacy of a child's behaviour to
lose weight — are beliefs based on factual knowledge and on
interpretations of past events or experiences. In general, beliefs can be
influenced quite well. Furthermore, the perceived positive outcomes of weight
regulating parental behaviours can only be brought about under conditions of
sufficient response-efficacy regarding the child's behaviour, that
is, when the parental behaviours produce the desired change in the child's
behaviour. The knowledge about weight regulating parental behaviour, and how to
perform it, can also be modified as it only requires adequate basic
information processing and storage. Structured parenting refers to a
parenting style in which children are actively guided and given clear
directions for choices and behaviours, for example, concerning food
intake and physical exercise. The experience with this type of parenting is
also modifiable and can be changed by practising it. Structured parenting
is less likely the more parents tend to engage in a democratic
parenting style, i.e. have a parenting style in which children are stimulated
(or often just left) to make their own choices. A positive attitude with
regard to a democratic parental style is perhaps difficult to
change as it may be based on parental modelling and a history of
perceived reinforcement of that
style. The conclusions with regard to the factors' modifiability are depicted
in Table 5.1.
Next,
she will evaluate the effect size of the
causal factors in the process model. How strong is the effect on the outcome
variable? Changes in the first three variables in the
balance table are probably possible but their effects on the outcome variable
largely depend on parents' perceived control over regulating
their children's weight. Just changing these variables may have a small
effect as only some parents will have
The
Help Phase 111
sufficient control beliefs. Changing the
knowledge on weight regulating parental behaviour can have a large effect, as it is
a primary condition to engage in such behaviour. Changing the positive attitude with
regard to a democratic parental style has uncertain effects, as it does not guarantee
that an adequate alternative style will be adopted. Changing the perceived control over
the child's behaviour can have large effects as it is a basis for developing
perceived positive outcomes of regulating the weight of one's children and perceived
control over this behaviour. Finally, experience with structured parenting can have various effects but it
does not guarantee that parents are skilled
in the specific behaviours regulating the weight of their children. A psychologist
will summarize her findings in the balance table (see Table 5.1).
From the balance table it appears that an
intervention that targets the knowledge on weight regulating parental behaviour
and the perceived control over a child's behaviour will probably be most successful. In
addition, a psychologist may also target the perceived negative outcomes of a
child being overweight, the perceived positive outcomes of the parental
behaviour, or the perceived response-efficacy of a child's behaviours.
DEVELOPING THE INTERVENTION
Once the psychologist has decided which variables to target, the
intervention can be developed.
Three tasks can be distinguished in the development of an intervention:
1.
Choosing
the right channel, in which way one may reach the target group
members for example.
2.
Selecting
the appropriate methods, the
way the changes will be brought about, for example, by offering a role model or performing a
skill exercise.
3.

 Developing
the strategies, the translation of the methods into concrete aspects of the
intervention. For example, when the method is social modelling, the strategy refers to the exact model and the things the model says and
does.
Developing
the strategies, the translation of the methods into concrete aspects of the
intervention. For example, when the method is social modelling, the strategy refers to the exact model and the things the model says and
does.
The channel, the method and the strategy must consider the target
group for intervention. A social
psychologist may focus on improving patient skill in taking a specific medicine when the target group consists of those
patients who already use, or who will use, that particular medicine. The choice
of channel is guided by the need to reach this target group (for example, through using a pharmacy) and by the method
(for example, modelling: watching another
patient taking the medicine on a DVD). The specific model (strategy) demonstrating the skills depends
upon the target group (for example, using an older model when the
patients are elderly). It is important to note that the development of an intervention is usually a dynamic process: choices for
the channel, the method and the strategy are made in combination (see
Figure 5.2).
The Channel
112 Applying Social Psychology
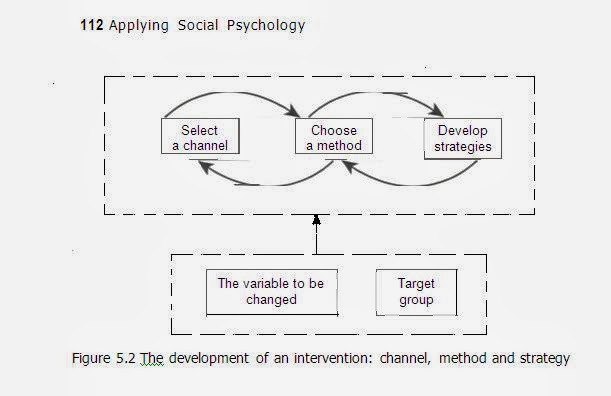
Figure 5.2 The development of an
intervention: channel, method and strategy
given of various channels and their
characteristics. Channels have several features,
and may vary from simple (for example, sticker or label) to
complex (for example, community intervention), each communicating a
distinct type of information (for example, text, picture) and a
different volume of information (for example, one simple message versus
a complex set of arguments). Some channels communicate with high intensity (say,
group therapy) and others with low intensity (say, information signs).
Channels
also differ in the potential reach of the
target group (see Table 5.2). For example, a label on a product has the
potential to reach all the users of a product, while a radio
message reaches only part of the population of users. In addition, some
channels will only have small effects on the
individual level (say, a sticker), while others can have large effects (the
example of group therapy). Lastly, channels may bring about different types of effects. For example, a label is
appropriate to increase people's knowledge, while counselling is more
appropriate to change complex and deeply rooted behaviours.
The
channel is chosen on the basis of information about the target group, the
relevant variables, methods and strategies. The following issues
should be considered when choosing the channel:
1.
Is the channel an effective way to reach the target
group? (See Table 5.3, potential reach.) When people want to know
how to use a product, say a wrist-exercise tool, using the label on
the tool works better than a television ad. The label ensures that people who
buy the tool have access to the information.
2.
Is exposure through this channel intensive
enough to change the variable? (See Table 5.2, effect
on individual level.) A billboard depicting a young woman during a physical
work-out may remind people that physical exercise is
desired, but may not lead to a change in attitudes toward working-out. Daily
feedback through the internet, however, may shape people's positive experiences with fitness, leading to the
desired changes.
Table 5.2 (Continued)
· CD-Rom/DVD Text,
pictures, sound, video, interaction Depends on the Medium New knowledge/
application2 Psychological change/
Behavioural
change
·
Internet/E-mail Information
sites,
interactive sites, People
with access to Small New
knowledge/
reminder mails, etc the internet Psychological/
change
Behavioural
change
· Cell-phone Reminder calls, SMS People
in the database Small Psychological
or all those who request change/
the service Behavioural
change/Reminder
· Television Commercials, infomercials, People who watch TV Medium New
knowledge/
documentaries, spots, etc channel at the time Psychological
of broadcasting change
· Minimal A few short personal contacts People who are Medium Psychological
counselling referred
to it change/
Behavioural
change
· Extensive Several or many personal contacts of People who are Medium/Large Psychological
counselling about
30-60 minutes referred to it change/Behavioural
change
· Group
training Education
and skills training in a group; People
who are Medium/Large Psychological
mostly 1 to 10 meetings referred
to it change/Behavioural
change
· Group
therapy Applying
therapeutic means to induce People
who are Large Psychological
change in individuals partly by means of referred to it change/Behavioural
Table 5.2 (Continued)
·
Regulations/laws
·
Structural environmental
changes
·
Community' intervention
|
Agreements about
permitted
or banned behaviours in more or
less specified contexts
Changing
the environment to regulate experiences or behaviours, e.g. by regulating the exposure to certain stimuli or
the availability of a specific product Changing peoples' experiences or behaviours by changing the structural and
informational
influences of the community they belong to
|
Depends on the application'
People who
encounter the specific environment
Members of the community
|
Large
Large
Small
|
Behavioural change
Behavioural
New knowledge/ Psychological change/ Behavioural
change
|
A
CD-Rom/DVD can be distributed in many ways. For example, they can be actively
sent to people who are registered in a database, they may be ordered
by those who feel they have a need for it or they can be distributed together
with product X.
3.
Is the channel appropriate for
the method and strategy? A sticker is less appropriate for modelling complex skills, such as learning to lead
a healthier lifestyle, while an interactive DVD gives several possibilities for modelling and practising healthy
skills. (See Table 5.2, effect type.)
The Method
Intervention methods also require consideration. Methods
are often derived from theoretical frameworks. For example, the foot-in-the-door
technique
(Cialdini & Trost, 1998), according to which people more easily accept a major request after first
complying to a minor request, is embedded in the theory
of self-perception that argues that people adjust their attitudes to their
behaviours (Bern, 1972). Such theories are important because they specify the conditions
under which the method is most or least likely to be successful. For example, according to social learning theory, modelling is most
effective when the similarity between model and target individual is high (Bandura, 1986).
From the various theories, phenomena and concepts in the Glossary (pp. 136-47) one can
often deduce ideas about methods.
Selection of a method
depends, first, on consideration of the balance table (see Table 5.1). For each variable,
an intervention method must be chosen. Suppose 'attitudes of police officers towards
foreigners' and 'communication with foreigners' are the selected variables to
improve the treatment of tourists in a city in Spain. Modelling might be used to demonstrate communication
skills, whereas the method of argumentation might target attitude
change. Second, selection of a method depends on the extent to which the method 'fits'
the variable one aims to change. Whereas some channels can motivate people to show
the desired behaviour, they cannot teach them how to change it. For example, it is
easy to arouse fear in smokers through a 30 second television advertisement, but it is
difficult to help them quit smoking using this channel. In contrast, it is
The Help Phase 117
often sufficient to remind people of the benefits of a certain
behaviour by using a prompt. For example, a sign on an elevator
door can prompt people to use the stairs for exercise.
The following methods are frequently used
in psychological interventions.
Goal
Setting
Setting
concrete and specific goals is important. Goals direct people's attention and effort,
provide them with expectations, and give the opportunity for feedback on goal accomplishment,
thereby regulating motivation. Goal setting changes behaviour by defining
goals that people must reach in a given period of time (Locke & Latham, 2002).
For instance, as regards being overweight, a goal can be set in terms of weight
loss in kilos over a particular time period. Sub-goals can help people
work on small, but important, steps in reaching the superordinate goal.
For example, in patients who have had a stroke, a goal in the
rehabilitation could be: 'After three months I can walk 200
metres by myself'. Many studies support the effectiveness of goal setting.
Evans and Hardy (2002) examined the effects of a five-week
goal-setting intervention for the rehabilitation of injured athletes. The
results showed that a goal-setting intervention fostered adherence and
self-efficacy. McCalley and Midden (2002) provided participants
with feedback to increase household energy conservation behaviour. They showed
that participants who had set goals for themselves eventually saved more energy.
Fear Communication
Fear
communication can be effective to motivate certain behaviours. For example, health
behaviours, such as using condoms, can be encouraged by graphic information about
sexually transmitted diseases (Sutton & Eiser, 1984). An interesting study
by Smith and Stutts (2003) compared the effects of a fear appeal showing
the cosmetic effects of smoking (unhealthy looking faces) with the
effects on one's health (cancer). They found that both fear-appeal conditions
effectively reduced smoking. It must be noted that fear communication is only
effective (and ethically justified) when it is accompanied by explicit
guidelines on how to avert the health threat.
Modelling
refers to learning through the observation of others. Watching others behave and
showing the consequences can teach people to perform a new behaviour (Bandura, 1986).
Modelling is useful for all kinds of skills, for example, coping with criticism,
cooking meals, and using condoms. In a meta-analysis, Taylor, Russ-Eft
and Chan (2005) examined the effects of different types of
modelling. Do people learn more when a skill is modeled positively (showing what
one should do), negatively (showing what one should not do) or in combination?
These psychologists concluded that skill development was greatest
when role models were mixed, that is, when they showed what one should
as well as what one should not do.
118 Applying
Social Psychology Enactive Learning
The most effective way of learning a skill is
to try to accomplish it yourself. This is called enactive learning. In interventions,
people can be stimulated to practise a certain skill and evaluate it. For
instance, to foster students' interest in science subjects like mathematics,
Luzzo and his colleagues (1999) exposed students to either a video presentation
of two university graduates discussing how their confidence in maths had
increased (so-called vicarious learning) or a maths task providing these
students with feedback on their maths skills (enactive learning). The
enactive learning condition proved more effective.
Social Comparison
Social comparison — information on how
others are doing — may affect one's mood and well-being (Buunk &
Gibbons, 2007; Festinger, 1954). For example, in the context of coping with
cancer, Bennenbroek et al. (2003) provided cancer patients undergoing chemotherapy
with social comparison information to increase the quality of their life. The
intervention consisted of a tape recording of fellow patients telling their
personal stories about either the treatment procedure, emotions
experienced during the treatment, or a tape about the way they tried to
cope with the situation. The latter tape especially reduced anxiety over
the treatment and improved patients' quality of life.
Implementation Intentions
Implementation intentions are intentions to
perform a particular action in a specified situation (Sheeran, Webb
& Gollwitzer, 2005). Sometimes people are asked to formulate their
implementation intentions. For a person who wants a low fat diet an
implementation intention could be: 'When I am at the supermarket I will
put the low-fat butter in the shopping trolley', or 'When I am at the party on
Friday night and somebody offers me cake, I will decline'. Asking
people about their implementation intentions may increase the occurrence of
desirable behaviours. Steadman and Quine (2004), for instance, showed that
asking participants to write down two lines about performing testicular
self-examination led to the desired action. Likewise, Sheeran and
Silverman (2003) compared three interventions to promote workplace health and
safety and found that asking people to write down their implementation
intentions was the most effective.
Reward and Punishment
In general, people repeat behaviours that are
followed by a positive experience (reward) while avoiding a negative
experience (punishment). In the smoking example, a reward may
take the form of a refund for the costs of a smoking cessation course from the health
insurance company, if people quit smoking for at least three months. In
contrast, the government may punish people for smoking by
increasing the price of cigarettes. Furthermore, people can learn to reward or
punish themselves. For example, people who succeed in refraining from smoking for a
week could treat themselves to a cinema visit. In general, there is much evidence
for the effects of punishment and rewards. Punishment of undesirable
behaviours (for example, high fines for drunk driving) works
The Help Phase 119
best when it is accompanied by rewards for desirable behaviours
(for example, praise for staying sober before driving) (Martin & Pear,
2003).
Feedback
Feedback on accomplishments is essential in behavioural change. People
losing weight want to know how
much weight they have lost. Without feedback people become uncertain and their motivation deteriorates
because they do not know whether they have made progress (Kluger & DeNisi, 1998). Brug and his colleagues
(1998) provided people with tailored computer feedback on their diet
(vegetables, fruit and fat intake) and on
dietary changes. Both feedback types appeared to improve dietary habits.
Likewise, Dijkstra (2005) showed that
a so-called fear appeal to smokers — a single sentence of individual feedback (It appears you are not aware
of the changing societal norms with regard to smoking') — was twice as
effective in reducing smoking as no feedback.
|
Box 5.2 Interview with Professor Gerjo Kok of the
University of
Maastricht (The Netherlands)
Maastricht (The Netherlands)
One of the oldest and most prominent application areas of social psychological theory is health. Professor Gerjo Kok is one of the leading scientists in this
field.
'In addition to research on the causes of unhealthy
behaviour, we have developed a process protocol,
called Intervention Mapping, that provides guidelines and
tools for the development of health promotion programmes. In certain ways
(Continued)
120
Applying Social Psychology
the protocol is like this
book. It helps social psychologists, health organizations and/or the
government to translate social psychological theory and research in actual health programme materials and
activities and develop health intervention programmes that are maximally effective. In general I see a great
future for applied social psychology. I believe that social psychology
will play a growing role in the solution
of societal and health problems. Especially with regard to the study of
unconscious processes (such as habits), the field of group dynamics, and the study of environmental determinants of behaviour
(such as social norms and social
control) I expect social psychologists to become (even) more active.'
Interested in Gerjo Kok's
research? Then read, for instance:
Dijkstra, A., De Vries, H., Kok, G. & Roijacker, J.
(1999). Self-evaluation and motivation
to change: Social cognitive constructs in smoking cessation. Psychology& Health, 14(4), 747-759.
Kok,
G., Schaalma, H.P., Ruiter, R.A.C., Brug, J. & van Empelen, P. (2004). Intervention mapping: A protocol for applying health
psychology theory to prevention programmes. Journal of Health Psychology, 9, 85-98.
|
The Strategy
Methods have to be
translated into a specific strategy. The strategy is the actual intervention
people will get exposed to. For example, using television as the channel and modelling as the method, the
strategy would specify the age and gender of the role model. In the case of flu
vaccinations for elderly people, the strategy might be a television spot ad in
which viewers watch an older woman, with good health, being interviewed in her doctor's waiting room, before
having her vaccination.
To come up with strategies, a global
intervention plan could be made specifying the methods, channels, target groups, and
variables to be changed as identified on the basis of the balance table. Here are some examples:
·
Modelling (method) on television (channel) to motivate women
with overweight children (target group) to monitor
their children's body weight (variable to be changed).
·
Giving feedback (method) through the internet (channel) about
the length of time youngsters (target group) engaged
in exercise during the past week to support an increase in their physical stamina (variable to be changed).
·
Offering arguments (method) to motivate quitting smoking (variable to be changed) in a self-help book (channel) for
smokers of all ages (target group).
·
Repetition (method) of the word 'action' in the text of a model (method) presented in a leaflet (channel), designed
to motivate obese people (target group) to
formulate implementation intentions with regard to
reserving a seat with extra space (variable to be changed) on international flights.
The Help Phase 121
Next, based on these global intervention
descriptions, the social psychologist could select
a strategy for intervention. This usually takes place in two phases, a
divergent and convergent phase. In
the divergent phase, the psychologist lists as many strategies as possible.
In the convergent phase, he or she critically evaluates these strategies.
The
Divergent Phase: Inventing Strategies There are various techniques to generate
interventions:
·
Direct intervention association. Ideas for strategies can be based on all kinds of
sources, such as what one has seen on television, what makes intuitive sense,
what has proven to be effective in the
literature or what people have experienced themselves.
·
Direct method approach. This approach consists of looking at strategies that have
been used in similar situations. For example, suppose that the global
intervention description is: 'Provide information
on the appropriate use of a new type of toothbrush on a label to prevent mouth
injury in patients with bad teeth.' A psychologist
might then inspect existing labels on toothbrushes. Also labels with regard to other devices that could injure
people could be used to generate ideas.
·
Debilitating strategies. This approach is to come up with strategies that have undesired effects
on the problem. In the case of the global intervention description: 'Modelling
on television to motivate women to monitor their children's weight', the model
should probably not be a retired millionaire
on his ranch. By generating ideas of what would probably have no or reverse effects, we can learn about what would
have an effect, about the relevant dimensions of an effective intervention and
about ways to operationalize the strategies.
·
Interviews. Interviewing
people from the target group could generate additional ideas for strategies.
With the global intervention description, 'Modelling on television to motivate
women to monitor their children's body
weight', a woman with young children might be interviewed about her
preference for role models that might inspire her. Here is an example of such
an interview:
'If there was to be an
intervention on television in which a person tried
to convince you that monitoring your children's body weight is important,
what kind of person would you trust most?'
'I think I would be persuaded most by someone with experience of
the problem. It should be a mother but knowing how things are manipulated on
television I would need to have proof that she really is a mother with experience.'
'Do you have any other ideas about the person and what
the person would say that would help you to accept the
message?'
'The mother should be a sensible person, with
some education. I think she should also be serious about the
topic; after all, it is about the health of your children.'
'What kind of person would you trust least?'
'When I got, one way or another, the
impression that they are indirectly
trying to sell a commercial product I would immediately stop watching.'
trying to sell a commercial product I would immediately stop watching.'
This kind of interview — asking for the
desired but also the undesired characteristics —can generate new perspectives and ideas about
strategies. From the above, we learn that people might feel they are being manipulated, which should of
course be avoided.
122 Applying Social Psychology
·
Insights
from theory. This approach consists of looking at relevant social
psychological theories. With regard to the
method of goal setting, for instance, the difficulty of the goal is crucial (Strecher, Seijts, Kok, Latham, Glasgow, DeVellis,
Meertens & Bulger, 1995). In general, goals stimulate performance
when they are difficult and offer a challenge but at the same time are within someone's reach. Losing two pounds in two
months might not motivate a person much, because the outcome is not very
attractive, but losing 20 pounds in two months might be unrealistic. Thus, in developing strategies, the
psychologist should look carefully at what the theory predicts.
·
Insights from research. This approach consists of looking at relevant social
psychological research. For example, research shows that people are less
defensive with regard to processing
threatening information (for example on cancer risks) when their self-esteem is
boosted (Sherman, Nelson & Steele, 2000). Therefore, in developing a
fear-appeal we might want to include a self-esteem boosting method, for example,
asking people to write an essay on the good
things they have done recently (Reed & Aspinwall, 1998). Such 'manipulations'
are described in the method sections of empirical articles and can
provide the social psychologist with creative
ideas for strategies.
The
Convergent phase: choosing the strategy
The divergent phase often results in a laundry list of strategies.
Therefore, a limited number of strategies need to be selected. The choice for a
particular strategy or set of strategies must have both a theoretical and empirical
basis. First the strategy should take into account the conditions underlying the
theory. For example, in the
case of modelling, the theory specifies that the actual model must be similar
or at least relevant to people in the target group (Bandura, 1986). Second, it
is preferable that the choice of strategy is based on
empirical evidence from either laboratory experiments or field studies.
Ideally, evidence ought to be available for the combination of the channel, the method, the strategy, the
variable to be changed and the
target group. For example, for the global
intervention description: 'Modelling on television to motivate women to monitor
their children's body weight', the strongest evidence would come from a field experiment
in which such an intervention was tested in a specified target group against a control condition.
Somewhat weaker evidence would come from
testing the intervention video in the laboratory. The stronger the
empirical evidence for the intervention, the higher the chances that the
intervention will indeed be effective.
Sometimes evidence for
the effectiveness of a certain strategy is simply not there. In that case, especially when the costs of an
intervention programme are high, we recommend that the effectiveness of a new
strategy should first be tested through research.
BUILDING THE
INTERVENTION PROGRAMME
The Help
Phase 123
graphic designer who is acquainted with the
technological possibilities, such as paper sizes, colour use,
lay-out, visual angles, and dynamic effects. Here are some rules of thumb
for preparing materials, based on our own experiences:
·

 Be as
specific as possible. In the case of a leaflet, formulate the final arguments,
write the introduction, link the arguments, and choose the font size and type.
In the case of a video with the method of modelling, write the script and
include what should be said and done and what should
happen in the video.
Be as
specific as possible. In the case of a leaflet, formulate the final arguments,
write the introduction, link the arguments, and choose the font size and type.
In the case of a video with the method of modelling, write the script and
include what should be said and done and what should
happen in the video.
·
 In the
case of an intervention with several channels (for example, billboards and
television spots) or sequential elements (for example,
group counselling sessions), all parts must be fine-tuned and a protocol must be written as well as with
planning the intervention.
In the
case of an intervention with several channels (for example, billboards and
television spots) or sequential elements (for example,
group counselling sessions), all parts must be fine-tuned and a protocol must be written as well as with
planning the intervention.
·
If professional artists are
involved, it should be clear how much influence they can have over the end-product. The communication with professional
artists should be highly interactive and several versions may
have to be designed by the artist in order to come up with a product.
·
The intervention often includes more than one
strategy. In principle, all aspects
of the intervention that can be read, seen or heard should be part of a
strategy. Thus, the colours, the sizes, the
sounds, the timing, the wording, the movement, the background, the aspects of
the background, and the specific
shapes should all refer to an identifiable strategy. One way to test
this is to point to a single aspect of the intervention and ask: What strategy
is this part of and what is the method of
operationalization?'
Pre-Testing the Intervention
Each planned intervention must be pre-tested. The
primary function is to improve the intervention and to avoid major flaws in the
design. A pre-test does not necessarily include a behavioural measure. It primarily
ensures that the target group will attend to the message as well as understand the
message. For example, to assess if people from the target group attend
to the persuasive message, they may be asked: 'Did you find the information
interesting?', 'Why did you find it not interesting?', and 'Were you still able to
concentrate on the message at the end?' In addition to such general questions, one
may add more specific questions. For example, when the social psychologist has
chosen a role model who is trying to persuade members of the target group,
there may be questions like 'How similar do you feel to the person
in the video?', 'How sympathetic do you find the person in the
video?', 'Did you believe the person on the video indeed
suffers from disease X, which he claims to do?', and 'What aspects of the model
should be changed for you to believe the person?'. The format of the
pre-test usually includes exposing a few target group members to the
preliminary intervention and assessing their reactions. This assessment
can be done in different ways.
· Interview. This
is in general a useful method to pre-test the intervention. One may have interviews
with individuals from the target group and ask questions like the ones above.
In addition, one may ask more specific questions.
For instance, people may be asked to read a leaflet and tell the interviewer
about their reactions, how reliable they found the information, how realistic
they
found it, and what they liked or did not like about the content or layout.
124 Applying Social Psychology
·
Quantitative assessment With
this type of pre-test, people from the target group answer closed questions about the intervention in a
questionnaire. For example, they may be asked to rate the reliability of the
source on a 7-point scale (from 'not at all reliable' (1) to 'very reliable' (7)) or they may be asked whether the intervention
'took too much time' , 'was just right' or 'was too short'. With a more
experimental paradigm, when one wants for example to use a sticker to indicate the location of the
fire-extinguisher in the building, this sticker could be pretested by comparing different versions.
·
Recall. The psychologist may also
use a recall task, which assesses which aspects of the intervention
people from the target group remember after having being exposed to the intervention.
This might give an insight into which strategies have the highest salience.
Imagine a billboard depicting a
celebrity promoting safe sex, but when individuals from the target group are
asked to recall the characteristics of the billboard, half of them only
remember the name of the celebrity and
not what he or she was promoting. In this case, the salience of the messenger has apparently distorted the message of
the intervention.
·
Observation: People from the target group may also be observed while
being exposed to the intervention. For example, in the case of
testing a billboard, eye movements may be monitored to track which aspects of the billboard they pay most attention.
Likewise, when testing an internet website, the link-choices and the time spent
on each page might be monitored.
·
Expert opinions For
pre-testing the intervention, one may also ask the experts involved in bringing about the effects of the intervention.
(For example, in the case of a leaflet to increase treatment adherence a
doctor might be asked to give his opinion.) Or a shop-keeper who is supposed to hand out a leaflet to everyone who
buys product X may be asked whether he or she thinks people will indeed look at
the leaflet.
In general, participants seldom agree
completely about an intervention in a pre-test. Therefore, an applied social psychologist must
not only look at the pre-test data, but must
also consider theoretical aspects as well as empirical evidence that may be relevant. After revisions have been made, the
improved intervention can be pretested
a second time. The final version of the intervention can now be developed and distributed.
IMPLEMENTATION OF THE INTERVENTION
When
the intervention has been developed the implementation process can start. The
implementation process has one major goal: to ascertain that the intervention
is used as intended. Thus, when a psychologist develops an
intervention campaign with leaflets and television advertisements, members of
the target group must be exposed to these messages. When all members are exposed to
the intervention (for example, they have all read the leaflet or have at least
seen one television advertisement), the intervention is
implemented optimally. Note that implementation is not about the effects of the
intervention but about positioning the intervention in such a
way that it can have its effects.
The core challenge of the implementation
phase is that the extent to which the target group is exposed to the
intervention depends on the people and organizations that are involved
in the distribution of the intervention. For example, with regard to a leaflet
The
Help Phase 125
Figure
5.3 Proportion of people who report needing the intervention programme, who
are aware of its existence, who have started using it and who have completed
the programme
about medicine intake, pharmacists may be
involved by motivating their employees to distribute the leaflet to all patients
getting a specific medicine. We cannot expect that all
these people are as motivated to get the target group members exposed to the
intervention as the initiators and developers of the
intervention. Therefore, the implementation of an intervention involves motivating others and removing
any perceived obstacles to allow them to
engage in their specific tasks.
Sometimes people who help
with the implementation are simply not aware of the intervention. Paulussen and his colleagues (1995; see also
Paulussen, Kok & Schaalma, 1994)
studied the implementation of an educational programme consisting of several lessons designed to promote AIDS
education in classrooms. Almost all the teachers had initially expressed an
interest in participating. Yet only 67 per cent of the teachers were aware of its existence on the
curriculum and only 52 per cent initially started to teach it. Although
Paulussen et al. (1995) did not assess whether the teachers finished a whole curriculum, this percentage
is likely to be substantially lower (see Figure 5.3).
Thus,
although psychologists may develop an excellent intervention programme, if only a
few people are actually exposed to the intervention because professionals who are
essential for its implementation, such as teachers or doctors, are not aware of
it or do not use it properly, the impact of the intervention
on the problem may be small or non-existent.
The
Implementation Process
126 Applying Social Psychology
dissemination
adoption
adoption
implementation
continuation
Figure
5.4 The diffusion process of innovations
large-scale changes in the use of an
innovation (for example, using a new toothbrush or using a new method to
quit smoking) take place in time. This process is referred to as the diffusion process. Rogers distinguishes four phases. We will
illustrate the process here with an example of a leaflet for battered women to
get professional help. This leaflet is to be handed out by general
practitioners if they suspect domestic violence.
1.
Dissemination phase. In this phase the general
practitioner becomes aware of the existence of
the leaflet on domestic violence and discusses it with colleagues.
2.
Adoption phase. In this phase the
practitioner becomes motivated to use the innovation and to hand out the leaflet to patients who are
suspected to be victims of domestic violence.
3.
Implementation
phase. In this phase the doctor actually engages
in the behaviour that will expose the target group to the intervention: he hands out
leaflets to the right patients.
4.
Continuation phase. In this phase handing out
the leaflet becomes normal practice.
In stimulating the diffusion process, all
four phases will have to be addressed: raising awareness among general practitioners,
motivating such practitioners to detect target group members (i.e., women who may be
victims of domestic violence), and to hand out the leaflet to these women, supporting the
practitioners in the actual execution of the behaviours, and providing feedback
and reinforcement to maintain the behaviours (for example, by calling
practitioners on the phone and giving them support and advice).
Note that the diffusion process highlights the phases in
the implementation process. It does not define all the parties that are
involved in the implementation, except for the end users of the innovation
(in the above example the general practitioners). The next step is to identify all the people
and organizations involved in the implementation process. For each of the four diffusion
phases, different people and organizations may be involved.
Mapping the
Implementation Route
The Help Phase 127
involved in the
implementation and their motivations and barriers to performing their task in the
implementation are mapped. Developing an implementation route consists of three steps:
1.
Mapping
the actors. The route shows the actors in the relevant networks in which they communicate and their means of communication. For
example, with regard to the implementation of: 'A leaflet with
information and arguments for battered women to get professional help',
individual general practitioners are members of a regional organization, which
is part of the national organization for
general practitioners. Within and between these levels of organization, individuals and organizations
communicate via different means, including for example, formal meetings,
professional journals and email. Furthermore, patients who read the leaflet
and decide to seek professional help should be able to make a first appointment
very quickly. Thus, the organizations
providing professional help to battered women must also be involved in
the implementation.
2.
Assessing the motivations and the barriers for actors. For a successful implementation, each of the actors will have to engage in a specific task. For
example, general practitioners should be
motivated to engage in detecting battered women and should dedicate some time
to this task. Furthermore, the board members of
a general practitioners' organization should be motivated
to invest some money in persuading general practitioners to perform the
detection or to persuade insurers that the detection
of battered women should be reimbursed. Thus the implementation
route contains for all actors a diagnosis of the potential problems to engaging
in the implementation's task and the specific barriers to performing it.
3.
Identifying relevant policies. Besides identifying the actors involved, the relevant
policies also need to be known. For example, it is possible
that there is a policy for general practitioners that says that the general
practitioner will not engage in detection tasks with regard to family matters. Although some general practitioners might
still be motivated, this would rot be an ideal situation for the implementation
of the intervention. Or it may be that there is a law that says that the police can only offer protection to a
battered woman when there is objective evidence
of domestic violence. This might inhibit women from seeking professional help.
This law would counter the desired effects of the intervention structurally.
The Implementation
Plan
When the actors,
organizations and policies have been identified and the motivation and the perceived
barriers to the actors have been mapped, the implementation plan can be
developed. The implementation plan consists of all the steps that should be
taken to stimulate the actors to conduct their task(s) in the implementation.
In developing
an implementation plan, the social psychologist must take two factors into account.
Implementation
Goals
For each actor or
level of actors and for each of the four diffusion phases, goals may he
formulated. For example, a goal for general practitioners in the first diffusion phase
could be: '80 per cent of the practitioners heard about the existence of the intervention
formulated. For example, a goal for general practitioners in the first diffusion phase
could be: '80 per cent of the practitioners heard about the existence of the intervention
128 Applying Social Psychology
material
on domestic violence and at least 50 per cent discussed the material with colleagues'.
On the organizational level, organizational goals should be formulated. For example,
a goal in the adoption phase could be: 'The board of the national organization for
general practitioners has decided to set aside one article in the professional
journal on domestic violence and to develop a pre-publication on it in their
communication with the regional organizations'. In principle, the goal
should be that every actor has a positive
attitude towards the implementation, or perceives their task in the implementation
as a legitimate part of their job.
Action Plans
Next,
the implementation plan specifies all the actions that must be taken to reach
the goals. This implementation manual specifies how
the goals can be reached. For example, the above goal with regard to
the awareness of general practitioners of the intervention
materials may be reached by actions directed at their national organization. For
example, we might want the board to be motivated enough to decide that some articles
on the detection of battered women should be published in their professional journal.
The Actual Implementation
The
actual implementation exists through executing the implementation plan. Thus, all
kinds of actions will have to be taken to inform and motivate the actors and to
take away
perceived or actual barriers for actors and to support the implementation. Actors may receive information designed to
motivate them, or permission to act from a higher level in their organization
or the means, in time or money, to do their part in the implementation. To support the execution of
the implementation tasks, the actors might
be contacted by e-mail, by letter, by telephone, by advertisements in professional journals, by presentations at meetings or
by their internal communication channels.
As may
be clear by now, the actual implementation of the intervention is time-consuming
and much work has to be done before any target group members will be exposed
to it.
The Evaluation
To
assess whether the problem that was targeted has indeed changed for the good, the
last step in this intervention-development cycle is to evaluate the effects of
the intervention. At least three types of evaluation are important: the effect evaluation, the process
evaluation and the cost-effectiveness
evaluation.
In the effect
evaluation, the extent to which variables that are directly related
to the problem have changed over time is assessed. At the very
least the effect of the intervention
The Help Phase 129
on the specified outcome variable in the process-model should be
assessed. There are, however, more outcome variables that may
be evaluated to determine the effectiveness of the intervention.
Imagine the case of the problem of obesity in which the level of
exercise is the variable that the social psychologist aims to influence. The
primary outcome variable in the process model is the level of
exercise. However, the number of people who engage in sufficient exercise
can also be a meaningful outcome variable. In addition, the
percentage of obese people six or 12 months after exposure to the intervention
could be an important outcome measure.
To
assess to what extent the effects are temporary or permanent, an appropriate follow-up
period must be specified. Long-term behavioural effects can be assessed 12
months after the exposure, although the 12 month period is based on consensus rather than on rationale.
The best follow-up periods are based on specific arguments for the behaviour that is targeted. For example, because in
smoking cessation most smokers who
relapse do so within the first six months after the initiation, a six
month follow-up should be sufficient; after this period very few ex-smokers
relapse.
In
the process evaluation, the
elements that are preconditions for the intervention to be
successful are assessed. There are two types of process evaluation. The primary-process evaluation refers
to an assessment of the changes in the variables that underlie the
changes in the outcome variables. For example, when the process model states
that prejudice towards Muslims is caused by media misrepresentations
of Muslims, the changes in prejudice as a result of unbiased publicity
might be assessed in a primary-process evaluation. In principle, all the
variables in the balance table that were targeted by
the intervention(s) are primary-process variables and may be evaluated. The secondary-process evaluation refers
to an assessment of the extent to which effective elements of the intervention
have indeed been executed. For example, for individual counselling
it may be essential that the counselor and the client develop a 'therapeutic
relationship' because the therapeutic relationship serves as one of the methods
of intervention. In a secondary outcome assessment, the extent to
which the therapeutic relationship has been formed is assessed.
In a cost-effectiveness evaluation the
costs of interventions are assessed and compared with the benefits.
For example, obesity has huge societal costs specifically in terms
of healthcare provision. If an intervention leads to a yearly decline of 500
people suffering from obesity, the healthcare savings can be
calculated. A second aspect of the cost-effectiveness concerns the costs of
intervention. The intervention development and implementation are
costly as they involve professional labour and material costs. For a television
advertisement to be broadcast, the costs for broadcasting must be paid. In the cost-effectiveness
evaluation the savings caused by the intervention are compared to the
costs of the intervention.
It
is important that for the effect evaluation as well as the cost-effectiveness
evaluation there are usually data sources available. Many
commercial research agencies gather information on societal phenomena.
such as the percentage of obese people and the number of unemployed. Thus, it may
not always be necessary to gather additional data. On the other hand, it is important that outcome
variables are carefully
130
Applying Social Psychology
Figure 5.5
Number of smokers (x 1000) 'as a function of type of channel' that were reached by the Millennium campaign 'I can do that too'
assessed.
Therefore, a self-developed outcome assessment may be necessary. Especially
with regard to the process evaluation, reliable measures must often be developed.
(For further reading on the evaluation of intervention we would refer to other
sources such as Action
evaluation of health programmes and changes by John Ovretveit,
2001.) In the last paragraphs of this chapter we present a case study of a large-scale
intervention that was successfully implemented to help smokers quit in the
Netherlands.
Case
Study: The Millennium Campaign 'I Can Do That Too'
In
the Netherlands, the Dutch Expertise Center of Tobacco Control developed the
Millennium campaign 'I can do that too' to reduce the percentage of smokers.
The campaign consisted of a series of interventions through
several channels to stimulate smokers to quit and support their attempt.
The campaign started in October 1999 and ended in February 2000.
The intervention programme is depicted in
Figure 5.5. In addition, the population was exposed to free publicity about the
campaign. In the written media, no less than 519 articles were published on the
Millennium campaign and 79 radio and TV items gave information on it.
The effectiveness of the campaign was
assessed using a so-called panel design with measurement control
groups (see Box 5.3). That is, before the campaign started, in October
1999 (Time 1), an initial measurement among smokers was conducted. This
The
Help Phase 131
group constituted the panel group. It is
common that such measurements may influence measurements done later
with the same group. If one finds a change in the panel group, this
could be an artefact of the first measurement (for instance, because it made
them aware of the risks of their smoking habits). Therefore, when the second
measurement was applied to the panel group (thus at Time 2, in
February 2000) there was also a control group of smokers with no Time 1
measurement. The same was done for the Time 3 measurement (January 2001).

In evaluating the effectiveness of the Millennium campaign, three outcome measures were used:
1.
seven-days' abstinence (not smoking for at
least the past seven days);
2.
having engaged in an attempt to quit;
3.
having positive intentions to stop smoking.
It was found that, at Time 2, those smokers
who had watched the TV programme or the TV talk show at Time 1 had made
significantly more attempts to quit. The long-term follow-up
(Time 3) showed that smokers who knew the Millennium campaign also had more positive intentions
to stop smoking. The researchers concluded that the Millennium campaign led more smokers to quit smoking and, for those who
had not yet made an actual attempt,
it had made smoking cessation a higher priority.
132 Applying Social Psychology
Developing an intervention programme includes the following steps: Box 5.4 The Help Phase: Developing an Intervention Programme
1.
Make a list of all the
causal variables in the process model and determine for each of them how modifiable they are and how large their
effect will (probably) be. Make a balance table to summarize the results.
Choose those factors for your intervention that are modifiable and that have
the greatest effect on the outcome variable.
2.
For each of the selected variables, come up with a channel, a
method and a strategy to influence this
variable. Justify your choices for the channels and methods and report on the use of different skills
to look for appropriate strategies
(i.e., direct intervention association, direct method approach, explore debilitating strategies, conduct interviews, look
at relevant theories and research).
3.
Reduce the potential list of strategies. In
selecting suitable strategies take notice of the conditions underlying the theory
that the particular strategy is based on
and look for research that supports the effectiveness of that particular
strategy. Develop the strategies you have chosen into an holistic intervention programme.
4.
Pre-test the intervention
programme by means of interviews, quantitative assessments, recall tests
or observations.
5.
Develop an implementation
route. Map the actors involved in the intervention's
implementation, assess the actors' motivations and the barriers they perceive,
and identify relevant policies.
6.
Develop an implementation plan. What steps
have to be taken to mobilize and motivate the actors
involved in implementing the intervention?
7. Implement
the intervention programme and evaluate its effectiveness.
SUGGESTED FURTHER READING
Bartholomew, L.K., Parcel, GS., Kok, G &
Gottlieb, N.H. (2006). Planning health
promotion
programmes: An
intervention mapping approach. San Francisco, CA: Jossey-Bass.
Ovretveit, J.
(2001). Action evaluation of health programmes and changes: A handbook for
a
user-focused
approach. Abingdon, UK: Radcliffe Publishing.
Rochlen, A.B., McKelley, R.A. & Pituch, K.A. (2006). A
preliminary examination of the 'Real Men, Real Depression' campaign. Psychology
of Men & Masculinity, 7(1), 1-13.
Smith, K.H. & Stutts,
M.A. (2003). Effects of short-term cosmetic versus long-term health fear appeals in anti-smoking
advertisements on the smoking behaviour of adolescents. Journal of Consumer
Behaviour, 3(2), 157-177.
Van Assema, P.,
Steenbakkers, M., Stapel, H., Van Keulen, H., Rhonda, G & Brug, J. (2006). Evaluation of a Dutch public-private
partnership to promote healthier diet. American
Journal of Health Promotion, 20(5), 309-312.
The Help Phase 133
ASSIGNMENT
5
A
company that produces computer software asks you, as a social psychologist, for
advice. The company consists of 10 departments, each of 50 employees,
with every department managed by an executive. These 10 executives
are in turn subordinate to a team of five directors that leads the
company. Although 50 per cent of the employees are female, of the
directors and executives only one person — the executive that runs the household
department — is female. The team of directors asks you how they can improve
the upward mobility of women in the company's hierarchy so the company will
have more female leaders in the future.
(a)
Read the following two articles:
Ritter,
B.A. & Yoder, J.D. (2004). Gender differences in leader emergence persist
even for dominant women: An updated confirmation of role congruity theory.
even for dominant women: An updated confirmation of role congruity theory.
Psychology of
Women Quarterly, 28(3), 187-193.
Eagly, A.H. & Karau, S.J. (2002). Role congruity
theory of prejudice toward female leaders. Psychological
Review, 109(3), 573-598.
Select from these articles causal factors and
develop a process model. Make sure that you limit the number of variables to
about 10 and don't take more than four steps back in the model.
(b)
Estimate for each causal factor in the
process model its modifiability and effect size. Make a balance table
and select the causal factors at which the intervention should be targeted.
(c)
For each of the selected factors, come up
with possible strategies to influence this factor. Use direct
intervention association and the direct method approach, explore debilitating
strategies, conduct interviews, and look at relevant theories and research.
(d)
Reduce the potential list of strategies by
examining their theoretical and empirical basis.
(e)
Outline a global intervention plan, a number
of ways to present the intervention and make a plan for the implementation of
the intervention.
(f)
Develop an evaluation procedure to determine
the effectiveness of the intervention programme
Menerapkan Psikologi Sosial Dari Masalah dengan Solusi
Abraham P. Buunk dan Mark Van Vugt


Komentar
Posting Komentar